
Abstract
Objectives:
The purpose of this paper is to describe the development and evaluation of a new medial linkage reciprocating gait orthosis (MLRGO) that incorporates a reciprocal mechanism and is sensitive to pelvic motion to potentially assist paraplegic patients to walk and provide functional independence.
Case description and methods:
The new orthosis was constructed and tested by a 20-year-old female paraplegic subject with transverse myelitis at T10 level, who was 4 years post injury and had also been an isocentric reciprocating gait orthosis (IRGO) user for 2 years. She received gait training for 12 weeks before undertaking gait analysis, and also completed a questionnaire that was designed to assess the perceived functionality of the new MLRGO when compared with an IRGO.
Results:
The results demonstrated improvements in gait velocity, step length and cadence, and also improvement in functional independence with the new orthosis compared with an IRGO.
Conclusion:
The results demonstrated that this new MLRGO could be used for paraplegic patients who would like an improvement in functional independence and ambulation.
Similar content being viewed by others


Introduction
Many assistive devices have been developed to provide standing and walking capability for people with lower-limb paralysis. Hip knee ankle foot orthoses (HKAFOs), reciprocating gait orthoses (RGOs) such as the Louisiana State University RGO, the Advanced RGO and the Isocentric RGO, plus medial linkage orthoses (MLOs) (such as the walkabout orthosis, Moorong orthosis, primewalk orthosis and the hip and ankle linked orthosis), are all orthoses that have been designed and used for paraplegic patients.1, 2, 3, 4 RGOs have produced improved gait parameters and lower energy expenditure than other devices,5 but they take a lot of time to don and doff and patients need assistance for standing and sitting. It has also been stated that they have an unacceptable appearance.6
In 1992, Kirtley and Mckay7 invented a new MLO that was designed to be positioned between two KAFOs and was lighter and less cumbersome than traditional or contemporary orthotic designs. One important advantage of this kind of orthosis is that the potential for independence in its donning and doffing. This MLO did not offer congruency between the anatomic and orthotic hip joints,8 which resulted in other kinds of MLO such as the prime walk and Moorong orthosis being designed,2, 3 but they do not offer a reciprocal mechanism or relative motion between the trunk and the lower limbs.
Studies have demonstrated the advantages of walking with an isocentric RGO (IRGO), such as less energy expenditure and improvements in gait parameters, when compared with MLOs.5, 9 On the other hand, the superiority of MLOs over RGOs in donning and doffing time and cosmetic appearance have been reported by paraplegia users.10 The design and construction of a novel mechanism that provides the combined characteristics of RGOs and MLOs has been recommended in literature in this field, and the aim of this study was therefore to design and evaluate the effect of a new reciprocating MLO on gait parameters and functional independence in a volunteer spinal cord injury subject.
materials and Methods
Case description and methods
A female patient (of age 20 years, weight 54 kg and height 165 cm) who had been suffering from transverse myelitis at T10 level for 49 months volunteered for this study. She was an experienced IRGO user with normal upper limb strength. The subject and her parents signed the agreement to participate form. The study was approved by the appropriate Ethics committee.
The mechanism incorporated in the new orthosis
The new device (Figure 1) incorporated two gears that were connected to bilateral KAFOs and also a saddle, plus a soft lumbosacral orthosis. During stance phase, when one leg is in an un-loaded position, the saddle-shaped plate of the orthosis rotates via posterior tilting of the pelvis. This rotation is transmitted to the case of the gearbox, turning the gear of the medial linkages backward and that of the swing linkage forward. Thus, the rotation of the saddle in an extension direction can provide hip flexion at the swing leg via the reciprocating mechanism.

New MRGO and IRGO.
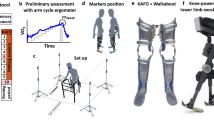
Experimental protocol
The patient walked through a 6-m-long calibrated space monitored by a 6-Camera Vicon digital motion capture system (Oxford Metrics, Oxford, UK) using a capture frequency of 100 Hz when wearing the IRGO (design and manufacture by Ortho system in motion company, Kirchheim, Germany) and the reciprocating link MLO (MLRGO) randomly in turn. Data were captured at a frequency of 100 Hz, as this is at least four times the frequency of walking data and is the accepted industry standard camera capture frequency commonly used in gait laboratories. Marker placements were set in plug in gait. For each test condition, the subject walked along the walkway five times between parallel bars.
To evaluate independence, a self-reported questionnaire was completed after completion of the gait training and a home trial period (Table 1). The time needed for donning and doffing of the orthosis was measured using a chronometer.
Results
Temporospatial and kinematic parameters
The MLRGO increased stride length, speed of walking and cadence by 5.45%, 33.3% and 27%, respectively, compared with the IRGO (Table 2). In addition, hip extension took more time but was nearer to that seen during normal hip movement than when walking with the IRGO (Figure 2).

The hip joint pattern of movement in the sagittal plane when using the two orthoses.
Independence
The patient demonstrated that she could don and doff the MLRGO independently when compared with the IRGO (where another person was needed). She could transform from sitting to standing and vice versa with the new orthoses, whereas she could not with the IRGO (Table 2).
Discussion
In this study, a new orthosis that combined all the advantages of RGOs and MLOs was evaluated. This design not only provided a link between the KAFOs for increasing stability,11 but also was sensitive to pelvic motion and moved the lower extremities reciprocally by using posterior pelvic tilt. It was also lighter than the IRGO tested (3 kg vs 6 kg) and could be used by the volunteer patient independently. The IRGO has been shown to be the most effective orthoses in improving gait parameters to date.5 This study showed that a new MLRGO can improve gait parameters compared with an IRGO. In addition, the IRGO uses rigid spinal orthoses for improved posture and uses trunk extension for hip flexion, but this rigidity limits range of motion in specific joints during walking. This new orthoses uses pelvic motion for hip flexion and does not need to incorporate a rigid trunk support but only uses a semi rigid trunk support, which may have produced the improvements in gait parameters noted. Lack of the need for a rigid trunk orthosis and using a medial hip joint instead of double laterally placed hip joints also reduced the weight of this orthosis.
The results showed that the MLRGO improved functional independency and reduced donning and doffing time because it does not have a rigid trunk component and hip joints. The patient could don and doff the MLRGO while is sitting on a wheelchair independently without any additional help, but when the patient used the IRGO she needed to lie down and needed another person to help donning and doffing. Also the functional independency questionnaire showed that the most differences noted between the two orthoses was its ‘usefulness for standing up in’. That is because unlike the IRGO, the MLRGO does not lock the hips joints but relies on subjects creating active and passive hip extension torques through hip and lumbar hyperextension, musculature and soft LSO, so does not create any restriction in the sitting to standing position.
Lack of a rigid LSO decreases orthosis weight and reduces limitation in ranges of motion, which will have contributed in allowing the patient to walk with improved gait parameters. This study therefore showed that all the spatiotemporal parameters tested were improved by the new design that could have been due to its lighter and more flexible structure, as well as it being sensitive to pelvic motion, whereas the IRGO is only sensitive to trunk motion.
Conclusion
An improvement in gait parameters and functional independence was demonstrated by one subject in this test study. Further evaluation is currently underway to assess the new MLRGO and its effect on gait parameters, stability and energy expenditure by a larger cohort of volunteer paraplegic patients.
Data Archiving
There were no data to deposit.
References
Genda E, Oota K, Suzuki Y, Koyama K, Kasahara T . A new walking orthosis for paraplegics: hip and ankle linkage system. Prosthet Orthot Int 2004; 28: 69–74.
Middleton J, Fisher W, Davis GM, Smith RM . A medial linkage orthosis to assist ambulation after spinal cord injury. Prosthet Orthot Int 1998; 22: 258–264.
Saitoh E, Baba M, Sonoda S, Tomita Y, Suzuki M, Hayashi A . A new medial single hip joint for paraplegic walkers. Ueda S, Nakamura R, Ishigami S. The Eighth World Congress of International Rehabilitation Medicine Association. Monduzzi Editore: Bologna, Italy, 1997, pp 1299–1305.
Whittle M, Cochrane GM, Chase AP, Copping AV, Jefferson RJ, Staples DJ et al. A comparative trial of two walking systems for paralysed people. Paraplegia 1991; 29: 97.
Arazpour M, Bani MA, Hutchins SW . Reciprocal gait orthoses and powered gait orthoses for walking by spinal cord injury patients. Prosthet Orthot Int 2012; 37: 14–21.
Ahmadi Bani M, Arazpour M, Farahmand F, Mousavi ME, Hutchins SW . The efficiency of mechanical orthoses in affecting parameters associated with daily living in spinal cord injury patients: a literature review. Disabil Rehabil Assist Technol 2014, 1–8.
Kirtley C, McKay S . Total design of the “Walkabout”: a new paraplegic walking orthosis. Proceedings of the Seventh World Congress of ISPO 1992. ISPO: Chicago, Illinois, USA., June 28–July 3. ISPO p39 [Abstract].
Onogi K, Kondo I, Saitoh E, Kato M, Oyobe T . Comparison of the effects of sliding-type and hinge-type joints of knee-ankle-foot orthoses on temporal gait parameter in patients with paraplegia. Japn J Compr Rehabil Sci 2010; 1: 1–6.
Harvey L, Davis GM, Smith MB, Engel S . Energy expenditure during gait using the walkabout and isocentric reciprocal gait orthoses in persons with paraplegia. Arch Phys Med Rehabil 1998; 79: 945–949.
Harvey LA, Smith MB, Davis GM, Engel S . Functional outcomes attained by T9-12 paraplegic patients with the walkabout and the isocentric reciprocal gait orthoses. Arch Phys Med Rehabil 1997; 78: 706–711.
Middleton JW, Sinclair PJ, Smith RM, Davis GM . Postural control during stance in paraplegia: effects of medially linked versus unlinked knee-ankle-foot orthoses. Arch Phys Med Rehabil 1999; 80: 1558–1565.
Acknowledgements
We thank the Iran National Science Foundation for financial support (grant number 9040942) for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Ahmadi Bani, M., Arazpour, M., Farahmand, F. et al. The influence of new reciprocating link medial linkage orthosis on walking and independence in a spinal cord injury patient. Spinal Cord 53 (Suppl 1), S10–S12 (2015). https://doi.org/10.1038/sc.2014.196
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.196
This article is cited by
-
The influence of new medial linkage orthosis on walking and independence in spinal cord injury patients: a pilot study
Spinal Cord Series and Cases (2016)
-
The influence of orthosis options on walking parameters in spinal cord-injured patients: a literature review
Spinal Cord (2016)
-
Comparison of new medial linkage reciprocating gait orthosis and isocentric reciprocating gait orthosis on energy consumption in paraplegic patients: a case series
Spinal Cord Series and Cases (2015)
